



- Home
/
- Stannous Fluoride
/
- Oral Health
/
Erosion Hypersensitivity

Erosion Hypersensitivity
Anti-Erosion
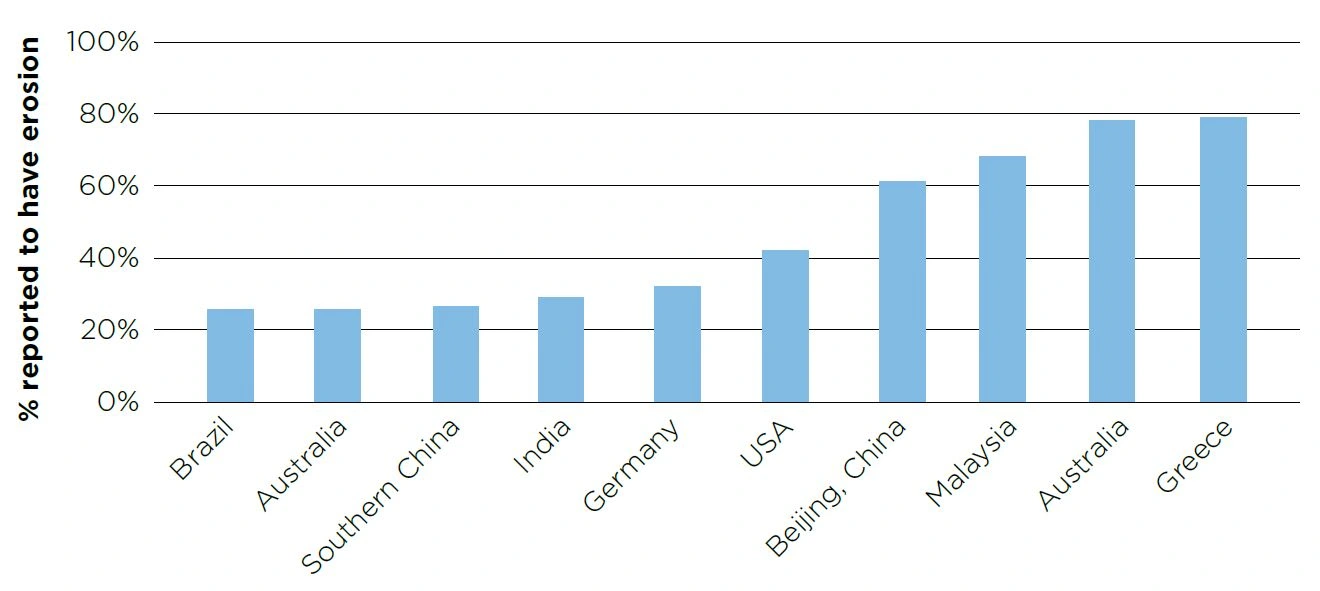
Dental erosion is prevalent in children and adults globally, with some researchers finding it present in approximately half of adolescents (Al-Dlaigan et al. 2001; McGuire et al. 2009). Estimated prevalence in some locations can be found in Figure 6.
Dental erosion is prevalent in children and adults globally, with some researchers finding it present in approximately half of adolescents (Al-Dlaigan et al. 2001; McGuire et al. 2009). Estimated prevalence in some locations can be found in Figure 6.
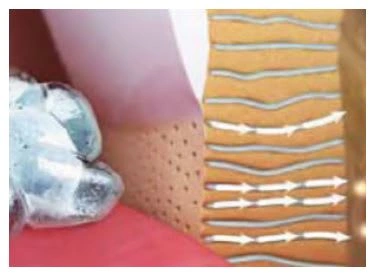
Dental erosion occurs primarily due to the excessive presence of non-bacterial extrinsic acids (especially dietary acids such as acidic drinks), as well as intrinsic gastric acid associated with gastroesophageal reflux disease (GERD) and bulimia (Moazzez et al. 2004; Bouqot & Seime 1997). Dental erosion involves the demineralization and softening of the tooth surface, which once softened, is highly susceptible to abrasion and attrition (Figure 7). A diagnosis of erosion can be made based on the pattern of surface loss of enamel and/or dentin (Figures 8a,b)
Figure 7. Demineralization associated with dental erosion

Figure 7. Demineralization associated with dental erosion
Figure 8a. Generalized erosion Courtesy of Prof. Ian Meyers

Figure 8a. Generalized erosion Courtesy of Prof. Ian Meyers
Figure 8b. Severe palatal erosion and loss of tooth structure. Courtesy of Prof. Ian Meyers

Figure 8b. Severe palatal erosion and loss of tooth structure. Courtesy of Prof. Ian Meyers
Unlike dental caries where demineralization is initially mainly subsurface and is also reversible in its early stages, dental erosion involves repeated demineralization of the surface with subsequent surface loss and this process is irreversible (Figures 9a, b).
Figure 9a. Dental caries process

Figure 9a. Dental caries process
Reversible Enamel crystals are weakened, but remain structurally intact. The early caries process is reversible
Figure 9b. Dental erosion process

Figure 9b. Dental erosion process
Irreversible Enamel crystals are damaged structurally from the surface down into the tooth. The erosive process is irreversible
Mechanism of action for anti-erosion effect of stabilized stannous fluoride
The deposition of stannous ions at the tooth surface helps protect it against dental erosion (Faller & Eversole 2014):
Deposition of stannous fluorophosphate or stannous oxide layers onto enamel surfaces has been reported after stannous fluoride treatment
Deposition occurs primarily as a result of the attachment of the stannous ion to free phosphate sites on the surface of enamel
Stannous forms a protective layer on the surface that is highly resistant to acids
A recent in vitro study compared the ability of various fluoride toothpastes to form a protective barrier layer (Faller & Eversole 2014). The toothpastes evaluated included 1,100 ppm stannous fluoride, 1,100 ppm sodium fluoride, 1,000 ppm sodium monofluorophosphate and 1,400 ppm amine fluoride. The study involved exposing etched samples to toothpaste-saliva slurries, rinsing them, and then exposing them to 2% alizarin Red-S. Dye deposition was assessed using a 5-point scale, with 0 being no dye deposition and 4 being complete dye coverage. A low score indicates a barrier layer is present, preventing the deposition of dye. The stannous fluoride toothpaste had the lowest score, 0.25. At the other extreme, amine fluoride resulted in a score of 3.7 (Figure 10). This in vitro test confirmed the ability of stannous to form a protective barrier layer, and demonstrated that stannous fluoride is a preferred fluoride for delivering an enamel protection benefit via a barrier mechanism to erosive acids.
Figure 10. Degree of dye deposition on enamel samples following exposure to toothpaste slurry followed by dye
* Average deposition of stain (based on the 5-point scale)

Other in vitro tests have also demonstrated the superior protective effect of stannous fluoride-treated enamel slabs in comparison to sodium fluoride-treated enamel slabs during an erosive challenge (Figure 11; Faller 2012). Exposure to dietary acid in an erosion cycling model resulted in surface demineralization and surface loss for the slabs treated with sodium fluoride toothpaste slurry while minimal demineralization or surface loss occurred with the slabs treated with stannous fluoride toothpaste slurry.

Figure 11. Stannous fluoride vs. sodium fluoride in in vitro treated enamel slabs

Erosion Research Summaries
The following study summaries represent a sample of research demonstrating the benefits of stabilized stannous fluoride dentifrice for protection against acid erosion.In addition, an independent consensus statement by the European Federation of Conservative Dentistry found “oral hygiene products, such as toothpastes or mouth rinses, containing stannous fluoride or stannous chloride have the potential to slow the progression of erosive tooth wear.” The authors found data are limited for other products. (Carvalho et al. 2015)
The Protective Effects of Toothpaste Against Erosion by Orange Juice: Studies In Situ and In Vintro
Reference: Hooper SM, Newcombe RG, Faller R, Eversole S, Addy M, West NX. J Dent. 2007 Jun;35(6):476-81. Epub 2007 Feb 27
CONCLUSION The results of this study provide further support for tooth brushing before meals. Results further suggest the stannous fluoride dentifrice could be used to provide significant erosion protection in susceptible patients versus that provided by conventional fluoride products.
Objective
Consumption of soft drinks, fruit juices and sport drinks has increased dramatically in the UK, the US, and elsewhere. Previous studies have demonstrated the erosive nature of these acidic soft drinks. The objective of this study was to determine the protective effects of experimental stannous fluoride-based toothpaste, containing sodium hexametaphosphate, against an erosive challenge (orange juice) on tooth enamel.
Materials and methods
This research included a 15-day challenge in vitro study and a 15-day in situ single blind, 3-way, crossover clinical trial.
The following formulations were tested:
experimental stannous fluoride dentifrice with sodium hexametaphosphate for cosmetic benefits (P&G);
a benchmark sodium fluoride dentifrice (CrestCavity Protection, P&G); and
negative control, water.
Flat, polished human enamel samples with a surface profile of +/-0.1μm, were exposed to the three regimens.
The orange juice used as erosion challenge had a pH 3.8.
15 volunteers wore an intra-oral appliance with 2 specimens of enamel embedded in the mid-palatal region from 9:00 to 17:00 (removed for 1 hour at lunchtime). Whilst appliances were in place, no food or drink other than water and the designated orange juice were consumed. Volunteers were asked to rinse with a toothpaste slurry or water at 9:00 and 13:00 followed by consumption of 250 ml orange juice 1 and 3 h later.
Subjects were treated with one study formulation for 5 days followed by two nontreatment days.
A profilometer was used to measure depths of the resulting eroded areas at days 5, 10 and 15.
Results
There was significantly more erosive damage on the specimens exposed to the benchmark toothpaste (NaF) and negative control (water) compared to the test stannous fluoride toothpaste in both the in situ (Figure 1) and in vitro (Figure 2) studies.
Figure 1. In Situ Loss of Material*

Figure 1. In Situ Loss of Material*
Figure 2. In Vitro Loss of Material*

Figure 2. In Vitro Loss of Material*
- mean value based on duplicate determinations of two enamel specimens
Enamel Protection vs. Abrasivity - A Study Of Relevance
Reference: Faller RV, Eversole SL, Tzeghai G. J Dent Res. 2009;88 (Spec Iss A): Abstract 3368.
CONCLUSION
- These results indicate
- the primary driver for enamel protection benefits is more likely the particular F salt, rather than RDA of the formulation. and
- this model is reproducible.
- Under the conditions of these studies, SnF2 provided superior protection against acid mediated enamel tooth surface loss.
Objective
Dentifrices with RDA< 250 are considered safe for daily use. Some researchers believe products with low RDA may be less aggressive on erosively softened enamel. Others believe that once softened, erosively challenged enamel will be removed by any friction, even by the tongue. This research was conducted to determine the primary driver of enamel protection benefits: is abrasivity or fluoride (F) salt the more important factor?
Materials and Methods
Cores of extracted, human enamel were cleaned, ground and polished to provide a virgin enamel surface, soaked in human saliva (pellicle formation), and treated in a 1:3 (product: saliva) slurry of toothpaste representing a range of actives/RDA values [SnF
2
(RDA~150), NaF#1(RDA~100), NaF#2(RDA~50)].
Specimens were subjected to dynamic pH cycling conditions including exposure to multiple 1% citric acid challenges over a 5-day period.
Treatment slurries and saliva baths were constantly stirred to ensure a steady flow, representing repetitive challenges to the enamel by a combination of common dietary acid and abrasive elements.
The study was run in duplicate to test model reproducibility. Results were averaged.
Results
The product with RDA~150 provided significant (P=0.05, ANOVA) protection against damage (8.0μm of surface loss), with lower RDA products (RDA~50 or 100) showing no significant differences between them in their ability to protect enamel against damage (27.3 and 25.4μm of surface loss, respectively). See Table and Figure.
It is important to note the active F species in the RDA~150 formulation was SnF2. SnF2 provides significant protection against erosive acid damage by forming a protective barrier layer on the enamel surface, protecting against external challenges.
The model is reproducible.
Table. Results

Figure Average % Reduction in Total Mineral Loss*
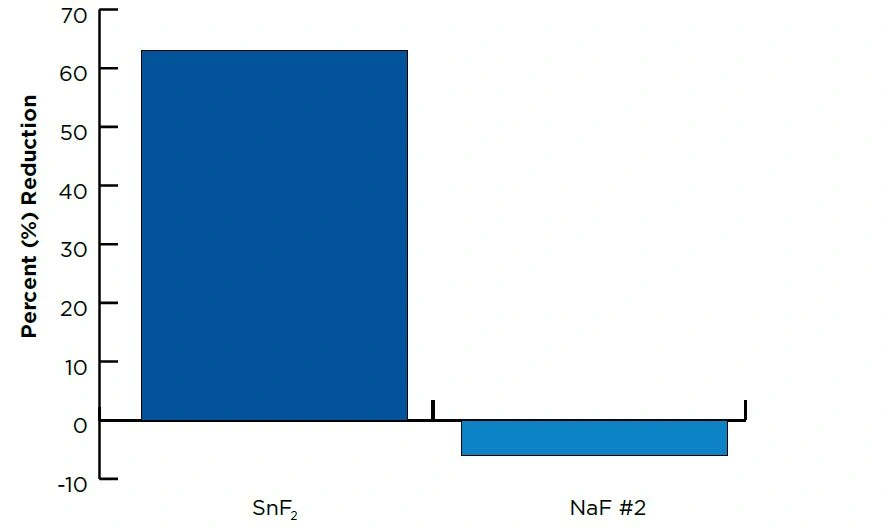
*(vs. NaF product)
A Randomized Clinical Trial To Measure The Erosion Protection Benefits Of a Stabilized Stannous Fluoride Dentifrice Versus a Control Dentifrice
Reference: XY Zhao1, T He2, Y He2, C Cheng2, HJ Chen2.1Fourth Military Medical University, Xi’an, PR China; 2Procter & Gamble.
Key clinical results
The experimental stabilized stannous fluoride (SnF2) dentifrice provided 26.9% greater erosion protection relative to the control dentifrice at Day 10 (P<0.03).
Figure. Treatment comparison at Day 10: Median Change in Enamel (μm)
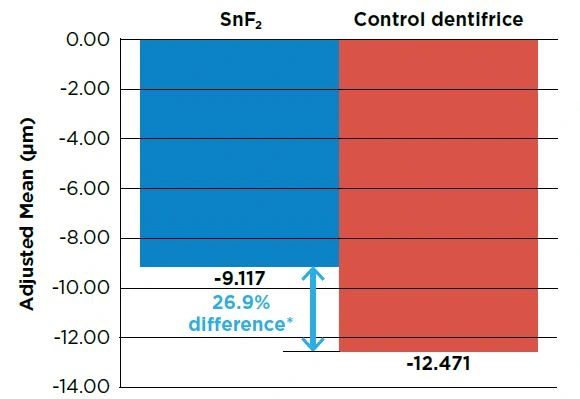
*Lussi A. Int Dent J 2014; 64 (Suppl 1): 2-3.
Objective
To compare the enamel protection efficacy of a stabilized stannous fluoride dentifrice and a marketed control dentifrice in a 10-day in situ erosion model.
Study design
A single center, double-blind, randomized, 2-treatment, and 3-period crossover clinical study was conducted involving healthy adults.
Subjects presented for 3 study periods and were randomized to treatment sequences, receiving one of the two marketed dentifrice products each period:
Experimental 0.454% stabilized SnF2 dentifrice (Crest® PRO-HEALTH™ Clean Mint [Smooth Formula], Procter & Gamble)
Sodium fluoride dentifrice with potassium nitrate marketed for protection from the effects of acid erosion (Sensodyne Pronamel, GlaxoSmithKline)
Each study period was comprised of 10 treatment days. On each treatment day, subjects brushed their teeth at home in their usual manner, using a non-treatment toothpaste and a regular, soft manual toothbrush supplied at the screening visit.
Subjects then attended the clinical trials unit where they collected their lower palatal intraoral appliance fitted with 8 enamel samples and placed it in their mouth. Subjects wore the appliance for approximately 6 hours total over the course of each study day. While wearing the appliance, subjects brushed their lingual teeth for 30 seconds, and swished with their assigned treatment toothpaste slurry for 90 seconds twice a day under the supervision of clinic staff.
The erosive challenge occurred with the appliance in the mouth. The subjects were required to sip 25mL of orange juice over a timed minute, swishing it around their mouth, then spitting out. This was repeated 10 times so that a total of 250mL of orange juice was exposed to the enamel samples over a 10 minute period. The erosive challenge occurred a total of four times on each treatment day.
On Day 10, the enamel samples were measured for tissue loss using a calibrated contact surface profilometer. Measurements were taken at baseline, prior to the start of the study, and at the end of treatment Day 10. Fresh enamel samples were placed in the intra-oral appliance at the beginning of each treatment period.
Statistical analyses utilized a general linear mixed model with period and treatment as fixed effects and subject as a random effect.
CLINICAL COMMENT
Stabilized SnF2 dentifrice has been shown to provide significantly greater protection from acid erosion compared to other types of fluoride dentifrice.* In this trial, a novel stabilized stannous fluoride dentifrice showed a significant anti-erosion benefit over a sodium fluoride/potassium nitrate dentifrice which is marketed for protecting enamel against acid erosion. Dental professionals should consider recommending this SnF2 dentifrice for its high level of protection against acid erosion as well as its benefits for reduction of gingivitis and plaque.
*Lussi A. Int Dent J 2014; 64 (Suppl 1): 2-3.
Clinical significance: Erosion

- The prevalence of dental erosion is increasing due to changes in the modern diet, which includes more acidic beverages.
- Dental erosion is irreversible and therefore must be prevented.
- The protective coating deposited on the tooth surface through the use of stabilized stannous fluoride dentifrice offers exceptional protection against erosion, making this dentifrice a suitable option for the prevention of erosion.
- Relative to other fluorides, stannous fluoride provides greater protection against enamel erosion.
Case studies

Patient Profile: Patient is 23__year old White Caucasian male.
Chief Complaint:“I need my front teeth to look good for my wedding pictures.”

Patient Profile: Patient is a 41year old White Caucasian female, 5’6” and weighs 165 lbs.
Chief Complaint: “My front teeth are sensitive to cold.”

Patient Profile: Patient is a 48year old White Caucasian female, 5’2” and weighs 110 lbs.__ Chief Complaint:__ “My teeth are really sensitive and my gums bleed when I brush my teeth.”

Patient Profile: Patient is a 42year old AfricanAmerican female, 5’6” and weighs 180 lbs. Patient reports she needs her teeth cleaned and has not seen a dentist in eight years.
Chief Complaint: “Some of my teeth hurt and my gums bleed when I brush my teeth. I have never had my teeth cleaned and I think this will prevent my bad breath.”

Patient Profile: Patient is a 38year old White Caucasian male.
Chief Complaint: “My teeth hurt and gums bleed frequently.”
Clinical studies

Randomized in situ clinical trial evaluating erosion protection efficacy of a 0.454% stannous fluoride dentifrice
Purpose: To assess the protective effects of a 0.454% stabilized stannous fluoride dentifrice and a marketed triclosan dentifrice against enamel erosion in a 10-day in situ model.

Determining the AntiErosive Effect of a Stannous Fluoride Containing Paste
Purpose: To determine the enamel protection efficacy of a stannous fluoride containing dentifrice compared to a conventional sodium fluoride containing dentifrice using a 10 day in situ erosion model.

The effects of different levels of brush end rounding on gingival abrasion: a double‑blind randomized clinical trial
Purpose: The objective of the study was to reapply simplified cycling model (SCM) to evaluate the demineralization potential of enamel for oral rinses.
Patient Education

SENSITIVE TEETH – CAUSES AND TREATMENT
Sensitive teeth (dentinal hypersensitivity) can occur when gums pull away from your teeth at the gumline exposing the dentin layer of your tooth.
Anti-Hypersensitivity
Mechanism of action of stabilized stannous fluoride dentifrice
Early treatments using solutions and later gels demonstrated the desensitizing effect of stannous fluoride. The dentinal tubules are occluded by precipitated stannous salts, inhibiting fluid movement within the tubules and thereby preventing nerve stimulation and pain (Figures 13, 14; Miller et al. 1994; Thrash et al. 1995).
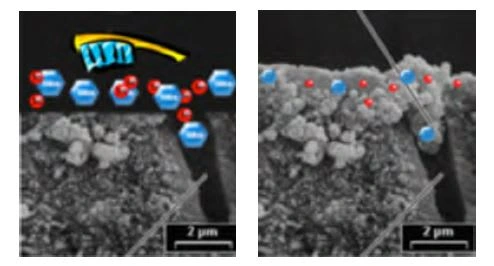
Figure 13. Dentinal tubule occlusion: Note the effective occlusion of dentinal tubules with stabilized stannous fluoride dentifrice (SEM x2000)

Figure 14. Pre-and post-brushing SEMs: pre-and post-treatment with open and occluded dentinal tubules Courtesy of Cosmetics & Toiletries

Figure 15. Relative dentinal tubule occlusion for stabilized stannous fluoride dentifrice versus two other anti-hypersensitivity dentifrices after treatment, mechanical agitation, and one minute acid exposure.

HYPERSENSITIVITY RESEARCH SUMMARIES
The following study summaries represent a sample of research demonstrating the benefits of stabilized stannous fluoride dentifrice for the reduction of hypersensitivity.
EFFICACY AND SAFETY OF A NOVEL STABILIZED STANNOUS FLUORIDE AND DENTIFRICE FOR DENTINAL HYPERSENSITIVITY
Reference: Schiff T, He T, Sagel L, et al. J Contemp Dent Pract. 2006;7(2):1-8.
CONCLUSION
Crest® PRO-HEALTH™ provided statistically significant reductions in dentinal hypersensitivity at 4 and 8 weeks compared to the sodium fluoride control dentifrice.
OBJECTIVE
To compare the efficacy of Crest® PRO-HEALTH™ vs a negative control dentifrice in the reduction of dentinal hypersensitivity over an 8-week period.
MATERIALS AND METHODS
Crest® PRO-HEALTH™ (a novel 0.454% stabilized stannous fluoride dentifrice with sodium hexametaphosphate for cosmetic benefits) was compared to a negative control dentifrice containing 0.243% sodium fluoride (Crest® Cavity Protection).
Study subjects were 90 generally healthy adults with moderate dentinal hypersensitivity: minimum of 2 bicuspid or cuspid teeth with sensitivity criteria of Yeaple Probe Index score = 10 g and Schiff Air Sensitivity Scale score of >1.
Experimental 0.454% stabilized SnF2 dentifrice (Crest® PRO-HEALTH™ Clean Mint [Smooth Formula], Procter & Gamble)
Tooth sensitivity was measured by tactile examination using the Yeaple probe (only teeth responding positively to 10 g and rechallenge at 10 g were evaluated) and cold air using the Schiff Air Index (teeth responding to air stimulus were evaluated).
Oral soft tissue examinations were performed.
Subjects were randomized to either the stabilized stannous fluoride dentifrice or the control dentifrice.
Subjects brushed twice daily with their assigned dentifrice using a manual soft toothbrush for 8 weeks.
Subjects were assessed again for sensitivity and safety at weeks 4 and 8.
RESULTS
Data were analyzed for all 90 subjects (45 in each treatment group).
Schiff Air Index scores were statistically significantly lower for the stabilized stannous fluoride group than the sodium fluoride control group at both weeks 4 and 8 (P<0.0001).
Compared to the sodium fluoride control group, the stannous fluoride group showed a 33% lower Schiff Air Index score (adjusted mean) than the sodium fluoride control group at week 4 and a 44% lower score at week 8.
Yeaple Probe Index scores were statistically significantly higher for the stabilized stannous fluoride group than the sodium fluoride control group at both weeks 4 and 8 (P<0.0001).
Compared to the sodium fluoride control group, the stabilized stannous fluoride group had a mean Yeaple Probe Index score 14 units higher (representing a mean desensitizing improvement of 114% greater) than that of the sodium fluoride control group at week 4, and 11 units higher (representing a mean desensitizing improvement of 71% greater) at week 8.
No adverse events were reported or observed.

Lower Schiff Air Index scores indicate less tooth sensitivity
DESENSITIZING EFFECT OF A STABILIZED STANNOUS FLUORIDE DENTIFRICE
Full text available in the Research Database at www.dentalcare.comReference: Schiff T, Saletta L, Baker RA, et al. Compend Contin Educ Dent. 2005;26(9 suppl 1):35-40.
CONCLUSION
Crest® PRO-HEALTH™ showed a clinically and statistically significant decrease in hypersensitivity compared to a negative control dentifrice.
OBJECTIVE
To evaluate the desensitizing properties of Crest® PRO-HEALTH™ compared to a negative control dentifrice.
MATERIALS AND METHODS
Crest® PRO-HEALTH™ (0.454% stabilized stannous fluoride dentifrice with sodium hexametaphosphate for cosmetic benefits) was compared to a marketed negative control dentifrice containing 0.243% sodium fluoride (Crest® Cavity Protection).
Study subjects were adults with a minimum of 2 bicuspid/cuspid teeth with sensitivity criteria of Yeaple Probe Index = 10 g and Schiff Air Sensitivity Scale score of >1.
Experimental 0.454% stabilized SnF2 dentifrice (Crest® PRO-HEALTH™ Clean Mint [Smooth Formula], Procter & Gamble)
Tooth sensitivity was measured by tactile examination using the Yeaple probe and thermal examination using the Schiff Air Index.
Oral soft tissue examinations were conducted and adverse events recorded.
Subjects were randomized to either the stabilized stannous fluoride dentifrice or the control dentifrice.
Subjects brushed twice daily with their assigned dentifrice using a manual soft toothbrush for 8 weeks.
Subjects were examined again for tooth sensitivity and safety at weeks 4 and 8.
RESULTS
Data were analyzed for 77 subjects who had complete data.
Yeaple Probe Index scores were statistically significantly higher for the stabilized stannous fluoride group than the sodium fluoride control group at both weeks 4 and 8 (P<0.0001). Higher Yeaple Probe Index scores indicate less tooth sensitivity.
Compared to the sodium fluoride control group, the stabilized stannous fluoride group had a mean Yeaple Probe Index score 1.6 times that of the sodium fluoride group at week 4 and 2 times at week 8.
Schiff Air Index scores were statistically significantly lower for the stabilized stannous fluoride group than the sodium fluoride control group at both weeks 4 and 8 (P<0.0001). Lower Schiff Air Index scores indicate less tooth sensitivity.
Compared to the sodium fluoride control group, the stabilized stannous fluoride group showed a 36% lower Schiff Air Index score (adjusted mean) than the sodium fluoride group at week 4 and a 44% lower score at week 8.
No adverse events were reported or observed.

Lower Schiff Air Index scores indicate less tooth sensitivity
A CLINICAL TRIAL EVALUATING IMMEDIATE SENSITIVITY RELIEF OF A 0.454% STANNOUS FLUORIDE DENTIFRICE
Reference: He, ML Barker, Qaqish J, et al. J Clin Dent 2011; 22: 46-50.
KEY CLINICAL RESULTS
The stannous fluoride (SnF2) dentifrice provided superior sensitivity protection relative to the negative control immediately after the first use based on the Thermal Schiff Index (13.8%, P<0.0001) and the Thermal Air Visual Analog Scale (14.6%, P<0.0001). See Figures 1 & 2.
The SnF2dentifrice also provided superior (P<0.0001) relief relative to the negative control at Day 3 and at Week 2 based on the Thermal Schiff Air Index (31.8% and 61.3%, respectively), the Thermal Air Visual Analog Scale (34.8% and 66.6%, respectively) and the Tactile Yeaple Probe (186% and 239%, respectively). See Figures 1 & 2 and Table 1.
The test products were well tolerated.
Figure 1. Thermal Schiff Air Index Adjusted Mean Scores (Lower score indicates less sensitivity)

Figure 2. Thermal Air Visual Analog Scale Adjusted Mean Scores (Lower score indicates less sensitivity)
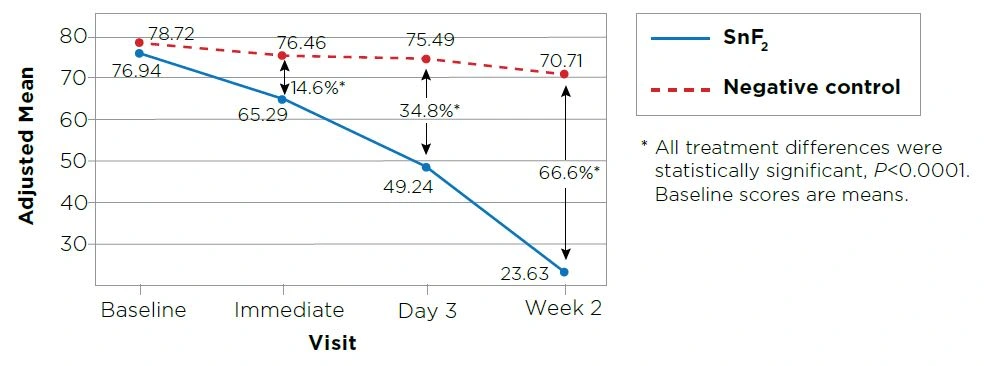
Figure 2. Mean tactile sensitivity scores at Baseline and Week 2. N=69

OBJECTIVE
To evaluate the efficacy of a SnF2 dentifrice in the reduction of dentinal hypersensitivity after immediate use, 3 days and 2 weeks of use as compared to a negative control dentifrice.
STUDY DESIGN
This was a controlled, randomized, examiner-blind, two-treatment, parallel group clinical trial.
One hundred eleven healthy adult subjects with moderate dentinal hypersensitivity were enrolled and randomized to one of two treatment groups.
Crest® PRO-HEALTH™ Advanced — 0.454% Stannous fluoride (1100 ppm fluoride), The Procter & Gamble Company, Cincinnati, OH.
At the Baseline visit, subjects received an oral soft tissue (OST) exam to evaluate the overall health of the mouth and then were reassessed for tooth sensitivity. Subjects with at least two sensitive teeth demonstrating reproducible sensitivity to both thermal and tactile stimuli and who met all eligibility criteria were enrolled in the study. For those subjects who had greater than two teeth meeting the eligibility criteria, only two were selected for enrollment in the study.
Subjects were then randomized to treatment (either Crest® PRO-HEALTH™ Sensitive Shield with 0.454% stannous fluoride, The Procter & Gamble Company or Colgate Cavity Protection dentifrice with 0.76% Sodium monofluorophosphate, Colgate-Palmolive). Products and treatment kits were identical in appearance to preserve blinding.
Subjects were instructed, according to manufacturer’s usage instructions, to brush with their assigned dentifrice thoroughly twice a day (morning and evening). Subjects in the stannous fluoride dentifrice group brushed the sensitive teeth first.
Subjects performed their first product use on site under the supervision of site staff. Immediately (within 5 minutes) following the first treatment, both the examiner and subjects re-assessed thermal sensitivity for each enrolled tooth using the Schiff Air Index (assessed by examiner) and Thermal Air Visual Analog Scale (assessed by subjects).
Safety and efficacy measurements, using Schiff Air Index, Thermal Air Visual Analog Scale and Tactile Yeaple Probe, were re-assessed at the Day 3 and Week 2 study visits.
A RANDOMIZED CLINICAL TRIAL EVALUATING A 2-STEP STANNOUS FLUORIDE DENTIFRICE AND WHITENING GEL SYSTEM VERSUS A POTASSIUM NITRATE DENTIFRICE FOR SENSITIVITY RELIEF
Reference: Gerlach RW, Underwood J, Miner M. Data on file, 2016.
KEY CLINICAL RESULTS
A 2-step stannous fluoride dentifrice and whitening gel system (Crest® PROHEALTH™ [HD]™, CPH-HD) provided superior tactile and thermal sensitivity relief (P<0.05) versus a positive control potassium nitrate dentifrice (Sensodyne® Extra Whitening). Both groups provided a significant benefit relative to baseline for both measures (P<0.0001). See Figures 1 & 2.
Seventy-two percent (72%) of teeth tested in the CPH-HD group experienced an improvement in thermal sensitivity compared to 53% in the positive control group. Fifty-five percent of teeth tested using the CPH-HD product experienced relief from tactile sensitivity compared to 37% for the positive control.
Figure 1. Mean thermal sensitivity scores at Baseline and Week 2. N=69
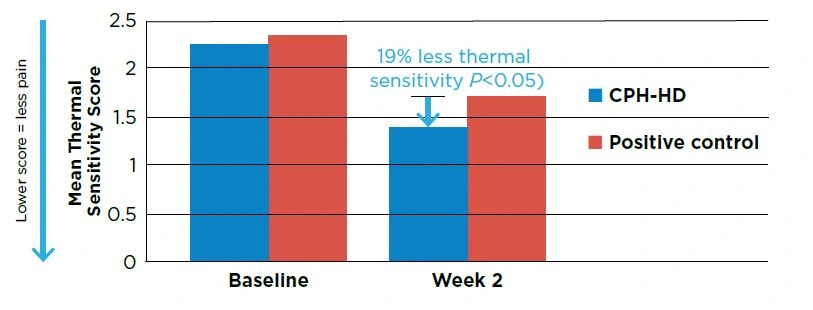
Figure 2. Mean tactile sensitivity scores at Baseline and Week 2. N=69

OBJECTIVE
To evaluate changes in dentinal hypersensitivity in response to using a two-step stannous fluoride dentifrice and whitening gel system relative to a positive control potassium nitrate sensitivity toothpaste.
This was a randomized, controlled, double-blinded study to assess changes in dentinal hypersensitivity over a 2 week period.
71 healthy adult volunteers with current dentinal hypersensitivity were enrolled and randomized to one of the groups for twice a day oral hygiene:
- Crest® PRO-HEALTH™ [HD]™: Step 1 is a 0.454% stannous fluoride dentifrice; Step 2 is a 3% is a hydrogen peroxide whitening gel (Procter & Gamble)
- Positive Control: Sensodyne Extra Whitening with sodium fluoride and 5% potassium nitrate (GlaxoSmithKline)
- Both groups used a soft, manual toothbrush (Oral-B® Indicator®, Procter & Gamble)
Assessment of dentinal hypersensitivity was made at baseline (before any treatment) and after 2 weeks of using the randomly assigned treatment using the Schiff Air Index1 (thermal) and Yeaple Probe2 (tactile).
Safety was assessed from clinical examination.
CLINICAL COMMENT Dentinal hypersensitivity is defined as a brief, sharp pain from the exposure of dentin to thermal, tactile, osmotic, chemical, or evaporative stimuli, which cannot be attributed to any other form of dental defect or disease. Patients commonly manage dentinal hypersensitivity by using a dentifrice containing a desensitizing agent, such as potassium nitrate or stannous fluoride. Potassium nitrate is reported to reduce sensitivity by interfering with the transmission of pain signals. Stannous fluoride has been shown to occlude open dentin tubules, reducing fluid flow in response to stimuli and thereby reducing pain.
Stabilized stannous fluoride dentifrice has been shown to provide superior relief from thermal and tactile dentinal hypersensitivity versus negative and positive controls.3 Consistent with published literature, the 2-step stannous fluoride dentifrice and whitening gel system provided superior sensitivity relief compared to a marketed potassium nitrate whitening dentifrice.* This 2-step system has also been shown to provide gingivitis reductions comparable to chlorhexidine* with significant whitening benefits.4,5 Thus, dental professionals can recommend this system to patients with dentinal hypersensitivity with confidence they will not only experience relief from sensitivity, but also improvements in gingival health and tooth whitening.
* via Step 1 stannous fluoride dentifrice 1 Schiff T, et al. J Clin Dent 1994;5 Spec No: 87-92. 2 Schiff T, et al. J Contemp Dent Pract 2006;May;(7)2:001-008. 3 Walters P. Dentinal Hypersensitivity: A Review. Updated Dec 2014; dentalcare.com CE Course #200. 4 Gerlach RW, et al. J Dent Res 2015;94 (Spec Iss A): Abstract 293. 5 Garcia-Godoy, C et al. J Dent Res 2016; 96 (Spec Iss A): Abstract 92.
CLINICAL SIGNIFICANCE: HYPERSENSITIVITY

- Given the high incidence of dentin hypersensitivity, the effectiveness of stabilized stannous fluoride dentifrice provides clinicians with an efficacious desensitizing dentifrice to recommend to patients.
- Stabilized stannous fluoride dentifrice offers anti-hypersensitivity benefits and provides multiple other important benefits concurrently with treating hypersensitivity.
- Stabilized stannous fluoride dentifrice provides both rapid and sustained sensitivity relief with continued use.
- In addition to rapid onset, the stabilized stannous fluoride dentifrice smear layer is resistant to acid challenges which occur through the modern diet.
CLINICAL STUDIES

Bioavailable gluconate chelated stannous fluoride toothpaste meta-analyses: Effects on dentine hypersensitivity and enamel erosion
Purpose: To compare the effect of bioavailable gluconate-chelated stannous fluoride (SnF2) toothpaste with control toothpastes for treatment of dentine hypersensitivity (DH) and enamel erosion.

A Randomized Clinical Trial to Assess the Desensitizing Benefit of a Stabilized Stannous Fluoride Dentifrice
Purpose: To assess the desensitizing efficacy of a stabilized stannous fluoride dentifrice versus a sodium fluoride negative control.

Fast onset sensitivity relief of a 0.454% stannous fluoride dentifrice
Purpose: To evaluate the efficacy of a stannous fluoride dentifrice as compared to a negative control dentifrice in the reduction of dentinal hypersensitivity after immediate use, and after three days and two weeks of use.

A Clinical Assessment of the Efficacy of a Stannous-Containing Sodium Fluoride Dentifrice on Dentinal Hypersensitivity
Purpose: To measure the desensitizing benefits of an experimental stannous-containing sodium fluoride dentifrice versus a regular sodium fluoride negative control.